Alpha-Tocopherol
Alpha-tocopherol is the most biologically active form of vitamin E, functioning as a lipid-soluble chain-breaking antioxidant that protects cell membranes from peroxidative damage.
Overview
Alpha-tocopherol is the predominant form of vitamin E in human tissues and the form preferentially maintained in the body by the hepatic alpha-tocopherol transfer protein (α-TTP). Structurally, it consists of a chromanol ring with antioxidant activity and a phytyl tail that anchors it within lipid bilayers. As a chain-breaking antioxidant, alpha-tocopherol donates a hydrogen atom to lipid peroxyl radicals, halting the propagation of lipid peroxidation in cell membranes and lipoproteins—a process central to atherosclerosis and cellular oxidative damage.
Dietary sources of alpha-tocopherol include wheat germ oil, sunflower seeds, almonds, hazelnuts, and vegetable oils. The recommended dietary allowance (RDA) for adults is 15 mg (22.4 IU) of natural alpha-tocopherol per day. Supplemental vitamin E is available as natural (RRR-alpha-tocopherol, formerly d-alpha-tocopherol) or synthetic (all-rac-alpha-tocopherol, formerly dl-alpha-tocopherol) forms, with the natural form having approximately twice the bioactivity per milligram. Large observational studies initially suggested that high vitamin E intake was associated with reduced cardiovascular disease risk, but subsequent randomized controlled trials, including the HOPE and ATBC studies, failed to confirm consistent cardiovascular benefit.
High-dose alpha-tocopherol supplementation (≥400 IU/day) has been a subject of controversy. A meta-analysis published in the Annals of Internal Medicine suggested a possible increase in all-cause mortality with high-dose supplementation, though the analysis has been criticized on methodological grounds. The tolerable upper intake level is set at 1,000 mg/day of any form of supplemental alpha-tocopherol. High doses may increase bleeding risk, particularly in individuals taking anticoagulant medications, due to alpha-tocopherol's inhibition of platelet aggregation and vitamin K-dependent clotting factors.
Mechanism of Action
Lipid Peroxidation Chain-Breaking
Alpha-tocopherol is the most biologically active form of vitamin E and the primary lipid-soluble antioxidant in human cell membranes. Its chromanol ring donates a hydrogen atom to lipid peroxyl radicals (LOO·), converting them to lipid hydroperoxides (LOOH) while forming the relatively stable tocopheroxyl radical. This chain-breaking activity halts the propagation of lipid peroxidation across polyunsaturated fatty acids in membrane phospholipids (PMID: 10543903).
Redox Recycling
The tocopheroxyl radical is regenerated to active alpha-tocopherol by ascorbate (vitamin C) at the membrane-cytosol interface, and subsequently by glutathione and lipoic acid, creating a cooperative antioxidant network. This recycling mechanism allows a relatively small pool of membrane-bound alpha-tocopherol to protect a large quantity of PUFAs (PMID: 11375433).
Non-Antioxidant Signaling Functions
Beyond radical scavenging, alpha-tocopherol modulates cell signaling through direct inhibition of protein kinase C (PKC) activity by competing for the diacylglycerol binding site. This suppresses smooth muscle cell proliferation, platelet aggregation, and monocyte adhesion. It also activates protein phosphatase 2A (PP2A), which dephosphorylates and inactivates PKC (PMID: 11157326).
Gene Expression Regulation
Alpha-tocopherol modulates expression of genes involved in inflammation and lipid homeostasis. It downregulates CD36 scavenger receptor expression on macrophages (reducing oxidized LDL uptake), inhibits 5-lipoxygenase and COX-2 transcription, and suppresses ICAM-1 and VCAM-1 expression on endothelial cells, reducing leukocyte adhesion (PMID: 12055337).
Ferroptosis Protection
Alpha-tocopherol is a potent inhibitor of ferroptosis, the iron-dependent form of regulated cell death driven by lethal lipid peroxidation, by trapping lipid peroxyl radicals in membrane phospholipids.
Reconstitution Calculator
Reconstitution Calculator
Calculate your peptide dosing

Set up a clean workspace with all supplies ready.
7x / week for weeks
This calculator is provided for informational and educational purposes only. It is not intended as medical advice, diagnosis, or treatment guidance. Always consult a qualified healthcare professional before preparing or administering any substance. PepGuide assumes no liability for decisions made based on these calculations.
Research
Reported Effects
Form Matters:: Natural D-alpha tocopherol appears more effective than synthetic forms, with users specifically seeking natural sources. Combination Synergy:: Vitamin E works best when combined with other nutrients like magnesium, vitamin K2, and selenium rather than as a standalone supplement. Limited Disease Prevention:: Clinical trials have not supported protective effects for cardiovascular disease or cancer prevention in adequately nourished populations. Tocotrienol Superiority:: Users and research suggest tocotrienols may offer superior anti-inflammatory and skin health benefits compared to alpha-tocopherol alone
- Natural D-alpha tocopherol appears more effective than synthetic forms, with users specifically seeking natural sources
- Vitamin E works best when combined with other nutrients like magnesium, vitamin K2, and selenium rather than as a standalone supplement
- Clinical trials have not supported protective effects for cardiovascular disease or cancer prevention in adequately nourished populations
- Users and research suggest tocotrienols may offer superior anti-inflammatory and skin health benefits compared to alpha-tocopherol alone
Safety Profile
Common Side Effects
- Gastrointestinal disturbances including nausea, diarrhea, abdominal cramping, and flatulence, particularly at doses exceeding 400 IU/day.
- Fatigue and muscle weakness with chronic high-dose supplementation (above 1,000 IU/day).
- Headache and blurred vision at supratherapeutic doses.
- Skin rash (contact dermatitis) with topical formulations in sensitized individuals.
- Easy bruising due to antiplatelet effects, particularly at doses above 800 IU/day.
Contraindications
- Vitamin K deficiency or concurrent anticoagulant therapy (especially warfarin): Alpha-tocopherol at high doses significantly increases bleeding risk by antagonizing vitamin K-dependent clotting factors.
- History of hemorrhagic stroke: The SELECT trial and meta-analyses have shown increased hemorrhagic stroke risk with vitamin E supplementation (approximately 22% relative increase in one large meta-analysis).
- Retinitis pigmentosa: High-dose vitamin E (above 400 IU/day) may accelerate vision loss.
- Known hypersensitivity to tocopherols or formulation excipients.
- Scheduled surgery: Discontinue at least 2-4 weeks prior due to antiplatelet effects.
Drug Interactions
- Warfarin and other anticoagulants: Alpha-tocopherol potentiates anticoagulant effects by inhibiting vitamin K-dependent carboxylation; INR may increase unpredictably. This is a clinically significant and well-documented interaction.
- Antiplatelet agents (aspirin, clopidogrel): Additive bleeding risk.
- Statins combined with niacin: Concurrent antioxidant supplementation (including vitamin E) reduced the beneficial HDL-raising effects of statin-niacin therapy in the HATS trial.
- Cyclosporine: Vitamin E may increase cyclosporine bioavailability.
- Chemotherapy and radiation: Antioxidant properties may theoretically reduce efficacy of pro-oxidant cancer treatments; concurrent use during active treatment is generally discouraged.
- Iron supplements: Vitamin E may impair iron absorption; separate dosing by at least 2 hours.
- Orlistat and cholestyramine: Reduce fat-soluble vitamin absorption, including vitamin E.
Special Populations
- Pregnancy: RDA (15 mg/day) is considered safe; high-dose supplementation is not recommended due to limited safety data and potential bleeding risk.
- Neonates: Intravenous vitamin E in premature infants has been associated with necrotizing enterocolitis and sepsis.
- Elderly: Increased all-cause mortality has been associated with high-dose vitamin E (≥400 IU/day) in meta-analyses; low-dose supplementation is generally preferred.
Monitoring
- INR/PT in patients on anticoagulant therapy.
- Serum alpha-tocopherol levels (reference range: 5.5-17 mg/L).
- Coagulation parameters before and during high-dose supplementation.
- Lipid panels if combining with statin therapy.
- Signs of bleeding or excessive bruising.
Pharmacokinetic Profile
Alpha-Tocopherol — Pharmacokinetic Curve
SubcutaneousQuick Start
- Typical Dose
- 400 IU (D-alpha tocopherol) is the most commonly reported dose for general supplementation
Molecular Structure
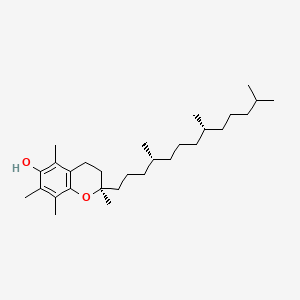
- Formula
- C29H50O2
- Weight
- 430.7 Da
- PubChem CID
- 14985
- Exact Mass
- 430.3811 Da
- LogP
- 10.7
- TPSA
- 29.5 Ų
- H-Bond Donors
- 1
- H-Bond Acceptors
- 2
- Rotatable Bonds
- 12
- Complexity
- 503
Identifiers (SMILES, InChI)
InChI=1S/C29H50O2/c1-20(2)12-9-13-21(3)14-10-15-22(4)16-11-18-29(8)19-17-26-25(7)27(30)23(5)24(6)28(26)31-29/h20-22,30H,9-19H2,1-8H3/t21-,22-,29-/m1/s1
GVJHHUAWPYXKBD-IEOSBIPESA-NSafety Profile
Common Side Effects
- Generally Well Tolerated:: Minimal side effects reported at standard doses, with vitamin E considered one of the safer fat-soluble vitamins
- High Dose Concerns:: Some research suggests very high doses may have pro-oxidant effects rather than antioxidant benefits
- Drug Interactions:: Potential interactions with anticoagulant medications due to vitamin E's effects on blood clotting
- Synthetic Form Issues:: Users express concerns about synthetic alpha-tocopherol (dl-alpha) versus natural forms (d-alpha), particularly in fish oil supplements
References (3)
- [1]Natural forms of vitamin E: metabolism, antioxidant and anti-inflammatory activities and the role in disease prevention and therapy
→ Review examining how different vitamin E forms (tocopherols and tocotrienols) have unique antioxidant and anti-inflammatory properties, with gamma-tocopherol and tocotrienols showing superior effects compared to alpha-tocopherol in certain disease prevention applications.
- [2]Vitamin E (α-Tocopherol): Emerging Clinical Role and Adverse Risks of Supplementation in Adults
→ Clinical review examining both the therapeutic potential and safety concerns of alpha-tocopherol supplementation in adults, noting limitations in primary disease prevention despite its antioxidant properties.
- [3]Alpha-tocopherol: roles in prevention and therapy of human disease
→ Comprehensive analysis revealing that alpha-tocopherol functions beyond simple antioxidant activity, also demonstrating pro-oxidant, cell signaling, and gene regulatory functions in various physiological processes.
Alpha-MSH (α-Melanocyte-Stimulating Hormone)
Alpha-melanocyte-stimulating hormone (alpha-MSH) is an endogenous tridecapeptide produced by post-translational processing of proopiomelanocortin (POMC) in the
American Ginseng
American ginseng (Panax quinquefolius) is a medicinal herb containing bioactive ginsenosides that undergo gut microbiota-mediated biotransformation into more po